
INDUSTRY GUIDES
Uncover key healthcare hiring challenges, including necessary OIG exclusion checks and the complexities of background verification.
Created by

Persistent nurse staffing shortages and urgent staffing demands in healthcare create daily pressure to compress or bypass legally required screening steps, exposing facilities to OIG Civil Monetary Penalties, FCRA class action liability, and Joint Commission accreditation risk. This article provides a compliance workflow model, grounded in federal regulatory requirements, that allows healthcare HR teams to meet screening obligations without sacrificing hiring speed.
Healthcare hiring challenges are not new, but the compliance risks embedded in urgent hiring decisions have never been higher. When a shift opens at 6 a.m. and a clinical manager needs a licensed RN on the floor by 7 p.m., the temptation is to treat compliance steps as bureaucratic friction rather than patient safety infrastructure. That framing is wrong, and it is expensive.
The U.S. faces a projected shortage of millions of healthcare workers over the next several years. Vacancy rates at hospital systems remain persistently elevated, and the regulatory penalties for hiring missteps in this environment are not theoretical. They are enforced. This article is written for the HR director, credentialing manager, or staffing coordinator navigating urgent staffing in healthcare who already knows the rules and needs a workflow model that makes compliance survivable at speed.
Healthcare hiring challenges in the compliance context refer to the operational conditions, including persistent staffing shortages and shift-fill emergencies, that pressure employers to compress or skip legally required screening steps, creating regulatory liability, patient safety risk, and potential class action exposure that urgency does not legally excuse.
Federal workforce projections indicate healthcare occupations are expected to add more jobs than nearly any other sector through the early 2030s. An AHA analysis of EMSI workforce data projected a shortage of up to approximately 3.2 million healthcare workers by 2026, with nurse staffing shortages representing the largest single segment of the gap. The structural shortage generates daily urgent staffing emergencies in healthcare facilities rather than occasional gaps.
The compliance collision happens at a specific inflection point: sequential hiring workflows designed for 72-hour or longer hiring cycles do not compress gracefully under same-day or next-shift urgency windows. The default response is to defer screening steps and backfill documentation later. That response treats compliance as a filing exercise rather than a liability firewall, and it misunderstands which obligations are time-invariant.
Some elements of the hiring workflow are compressible. The time between posting a position and scheduling an interview can be eliminated in an urgent scenario. Pre-employment paperwork can be sent electronically at the point of verbal offer. Reference calls can be deferred for non-clinical roles that do not involve direct patient care.
The following steps, however, do not compress regardless of urgency:
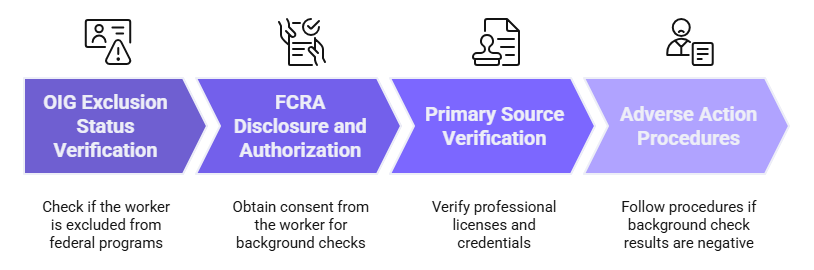
The distinction between compressible and non-compressible steps is the core of the workflow engineering problem. When HR teams treat all steps as equally compressible under time pressure, they tend to eliminate the non-compressible ones first because those steps have external dependencies that feel like delays. The result is not a faster hire. It is a compliant-looking hire that carries regulatory liability.
Healthcare environments also carry a specific standard-of-care dimension that general employment compliance does not. An unscreened worker providing direct patient care is not only a regulatory exposure. That worker represents a chain-of-custody gap in the organization's duty to protect vulnerable patients. The Joint Commission, CMS Conditions of Participation, and state licensing boards each impose independent obligations that exist alongside, not instead of, federal employment law requirements.
Important: Urgency does not create a safe harbor, a deferral window, or an emergency exception to federal or state compliance obligations in healthcare hiring. The obligations described in this article attach at the point of employment or service provision.
The OIG List of Excluded Individuals and Entities (LEIE) is the federal database maintained by the HHS Office of Inspector General. It identifies individuals and entities excluded from participation in Medicare, Medicaid, and other federal healthcare programs. A facility that employs, contracts with, or arranges for the services of an excluded individual in a role that provides items or services billable to a federal healthcare program faces Civil Monetary Penalty exposure regardless of whether the facility knew the individual was excluded.
The penalty structure scales. Under the applicable federal statute governing Civil Monetary Penalties, the OIG has authority to impose per-item penalties and assessments that can accumulate quickly when an excluded individual has provided multiple billable services before discovery. In home health or long-term care contexts where a single worker may generate dozens of billable visits per month, cumulative exposure from a single undetected exclusion can be significant.
The OIG's enforcement record confirms this exposure is not hypothetical. The agency has taken action against home health agencies and other healthcare providers for employing excluded individuals, and enforcement activity covers community-based and outpatient settings, not only acute care hospitals.
The misconception driving most skip behavior is that urgency creates an implicit deferral window: run the check after the first shift, before the first payroll cycle, or before the first billing submission. OIG guidance does not support that interpretation. Liability arises at the point of employment or contracting, when services are furnished by the excluded person. A facility cannot un-provide the services that occurred during a deferral window after the exclusion is discovered.
Note on Emergency Exemption: A limited emergency exemption exists under 42 CFR 1001.1901(c) for certain emergency items or services not provided in a hospital emergency room. This exemption is narrow and does not apply to routine urgent staffing scenarios. Consult legal counsel before relying on this provision.
Running the OIG LEIE check is operationally straightforward. The search tool at exclusions.oig.hhs.gov allows a name-based search that returns results immediately. A complete individual search, including reviewing the result and documenting the outcome, takes under five minutes per individual. There is no technical bottleneck that justifies deferral.
For facilities with federal contracting relationships, the SAM.gov exclusions database supplements the LEIE and should be checked as well. SAM.gov covers a broader range of federal program exclusions, and both searches take comparable time.
License verification in rushed healthcare hiring fails at a specific point: the moment a credentialing manager accepts a candidate's own attestation, a photocopy, or a scanned license certificate as evidence of current licensure in good standing. None of these satisfy the primary source verification standard required by The Joint Commission under Human Resources Standard HR.01.02.01. None satisfy CMS Conditions of Participation requirements for facilities participating in Medicare and Medicaid.
Primary source verification means verification obtained directly from the issuing authority, which is the state licensing board or its authorized designee, confirming in real time that the license is current, active, and free of any disciplinary restrictions. A photocopy provided by the candidate reflects what their license looked like at the time the copy was made. Discipline flags are frequently added after a license is issued without invalidating the paper credential.
Joint Commission Standard HR.01.02.01: The Joint Commission requires primary source verification of licensure, certification, and registration prior to the practitioner providing care, treatment, or services. There is no exception for emergency staffing circumstances, temporary assignments, or agency-placed workers.
For registered nurses and licensed practical nurses, the fastest primary source verification pathway in most states is Nursys, the license verification system operated by the National Council of State Boards of Nursing. Nursys returns real-time license status, multistate compact coverage where applicable, and any discipline flags on record. The query returns results immediately and is accepted by accrediting bodies as a primary source confirmation.
Physician verification follows a different pathway. State medical boards maintain individual license records. Most state medical board license lookups are available online and return results within minutes for straightforward queries. For locum tenens placements involving multistate licensure, physician records require particular attention because a physician may hold licensure in multiple states with varying discipline histories across boards.
The staffing agency assumption problem deserves direct attention. Many facilities operate under the belief that when a staffing agency provides a credential packet, the agency's verification satisfies the facility's primary source obligation. This belief is incorrect. The facility is the entity subject to Joint Commission accreditation audit and CMS survey. When a surveyor asks for primary source verification documentation, the facility's answer must be its own verification record. A facility that relies on an agency credential packet without independently confirming primary source compliance is exposed to adverse accreditation findings that the agency contract cannot cure.
FCRA liability in urgent healthcare hiring does not appear on the day of the hire. It surfaces weeks or months later when a candidate who was screened, declined, and never properly notified retains counsel, or when a pattern of adverse action procedure failures across multiple urgent hires attracts class certification. The urgency of the original hiring decision is not a defense.
The FCRA's application to temporary, per-diem, contract, and agency-placed workers is frequently misunderstood. Some facilities treat non-permanent workers as outside the FCRA framework because the employment relationship is structured differently. Any employer who procures a consumer report for employment purposes must comply with the full FCRA framework, including disclosure, written authorization, and the two-step adverse action process, regardless of the duration or nature of the employment relationship.
The two-step adverse action process requires that before taking adverse action based on information in a consumer report, the employer must provide the candidate with a copy of the report and a written summary of their rights under the FCRA, then allow a reasonable period for the candidate to respond before the adverse action becomes final. The FCRA does not specify a minimum number of days. FTC guidance and court decisions have generally treated a period of several business days as a defensible minimum, though employers should consult legal counsel for guidance specific to their jurisdiction and circumstances.
Class exposure develops not from a single adverse action failure but from a systematic pattern. When a facility applies a consistent practice of skipping or shortening the pre-adverse action notice period across multiple urgent hires, each instance can become a member of a potential class. Adverse action procedure failures are among the most commonly cited triggers for class certification in employment background screening cases.
The workflow fix is structural. FCRA disclosure and written authorization do not require the position to be filled first. They require only that the employer intend to procure a consumer report for employment purposes. Sending disclosure and authorization electronically at the point of verbal offer, before the shift start date and before the background check is ordered, compresses the timeline without eliminating any required step.
The EEOC's guidance on individualized assessment in background screening also applies in urgent hire scenarios. A facility that categorically excludes candidates based on background check results without conducting an individualized assessment of the nature of the offense, time elapsed, and nature of the position may face disparate impact exposure under Title VII in addition to FCRA exposure. Individualized assessment is a best practice and, in some jurisdictions, a legal requirement.
State Criminal History Reporting Rules: State laws governing what criminal history information can be reported in background checks vary significantly by jurisdiction. Rules in states including California, New York, Maryland, Massachusetts, Washington, and others impose lookback period limits, restrictions on non-conviction records, and other requirements that may apply based on where the applicant resides, where the employer is located, or where the underlying record originates. Employers and background check providers should apply the most conservative applicable standard. Confirm current state-specific rules with legal counsel or a PBSA-accredited consumer reporting agency.
The dual-accountability structure in agency placements is one of the most misunderstood compliance gaps in healthcare staffing. Facilities routinely assume that when a staffing agency delivers a credentialed worker, the agency's screening satisfies the facility's compliance obligations. That assumption is operationally convenient and legally incorrect.
The facility is the entity named in the CMS Conditions of Participation. The facility is the entity subject to Joint Commission accreditation survey. The facility is the entity that bills federal healthcare programs for the services rendered on its premises by agency-placed workers. When an OIG surveyor or CMS auditor asks whether an excluded individual provided billable services at the facility, the relevant question is not what the agency checked. It is what the facility verified independently before that individual began providing services.
| Obligation | Agency Responsibility | Facility Responsibility | Delegable? | Notes |
| OIG LEIE Exclusion Check | Yes, before placement | Yes, independently | No | Facility retains independent duty |
| SAM.gov Exclusion | Varies by contract | Yes, if federal contractor | No | Non-delegable for covered facilities |
| Primary Source License Verification | Yes, to agency standard | Yes, independently before care delivery | No | Joint Commission requires facility record |
| FCRA Disclosure and Authorization | Yes, if agency orders report | Yes, if facility orders supplemental report | Partial | Depends on who orders the consumer report |
| Adverse Action Process | Yes, for agency-ordered reports | Yes, for facility-ordered reports | Partial | Each reporting entity bears its own obligation |
| Ongoing Monitoring Post-Placement | Varies by contract | Yes, for duration of services | No | Facility bears ongoing exclusion monitoring duty |
What facilities should independently verify, even when relying on agency screening, includes: OIG LEIE exclusion status confirmed through their own search, SAM.gov exclusions if applicable, and primary source license verification through Nursys or the relevant state board. The documentation of this independent verification must exist in the facility's own credentialing file, not only in the agency's system of record.
Staffing agency agreements should explicitly define who runs which checks, what standard applies, and what the agency represents about the completeness and recency of its screening. However, contractual transfer of responsibility does not eliminate the facility's regulatory exposure. A contract clause stating that the agency bears full responsibility for exclusion verification does not satisfy a CMS auditor or provide a defense in an OIG enforcement action.
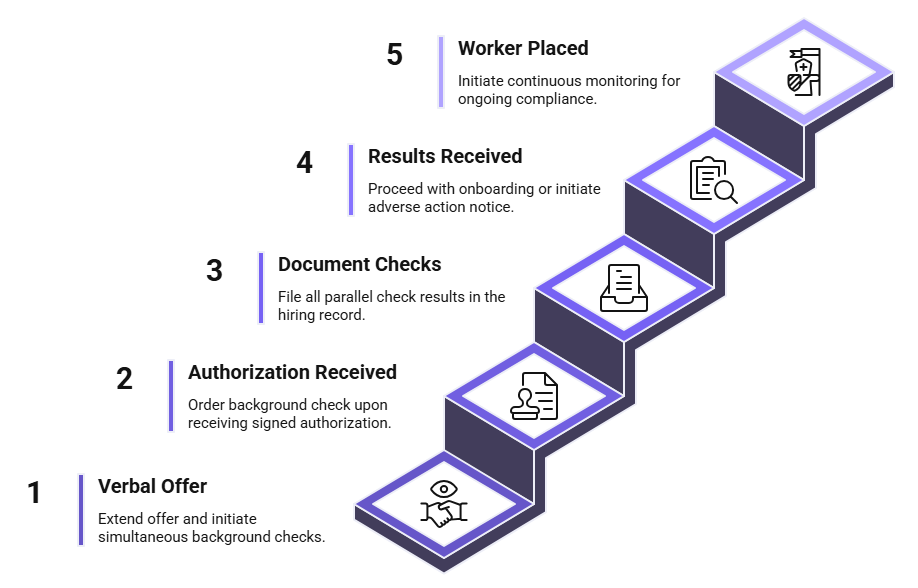
Sequential screening is the workflow architecture that makes urgent staffing in healthcare feel incompatible with compliance. In a sequential model, each step waits for the prior step to complete. Each handoff creates delay, and under time pressure those delays create the impulse to skip the slower steps.
Parallel sequencing reorders the architecture without removing any step. The critical insight is that most compliance steps have no dependencies on each other. The OIG exclusion check does not require a completed background report. License verification does not require FCRA authorization. FCRA disclosure can be sent before any other step is complete. The only hard dependency is that a background check cannot be ordered until signed FCRA authorization is received.
| Role Type | OIG LEIE | SAM.gov | Primary Source License | Criminal Background | Continuous Monitoring |
| Registered Nurse (per-diem or contract) | Required, pre-placement | If federal contractor | Nursys, pre-placement | Required, FCRA-compliant | Strongly recommended |
| Per-Diem Allied Health (PT, OT, RT) | Required, pre-placement | If federal contractor | State board, pre-placement | Required, FCRA-compliant | Strongly recommended |
| Locum Tenens Physician | Required, pre-placement | If federal contractor | State medical board, all active states | Required, FCRA-compliant | Required |
| Home Health Aide | Required, pre-placement | If federal contractor | State registry, pre-placement | Required; state-specific rules apply | Required |
Parallel sequencing does not make compliance faster by skipping steps. It makes compliance faster by eliminating the sequential handoff delays between steps that have no dependency on each other. Every required step still occurs. The total elapsed time is compressed because multiple steps run simultaneously rather than in series.
Urgency is a permanent feature of healthcare staffing, not a temporary condition. For facilities managing healthcare hiring challenges under real-time pressure, the compliance obligations are not suspended by workforce shortages, shift-fill emergencies, or the operational pressure of any given day. They attach at the point of employment or service provision.
The practical answer is not to slow down the hiring process. It is to redesign the workflow so that the required steps run in parallel rather than in sequence. An OIG exclusion check that takes five minutes, a Nursys verification that returns in real time, and FCRA disclosure sent electronically at the point of verbal offer together constitute a compliant hiring workflow that can run inside a compressed urgency window.
Facilities that document this parallel architecture, assign clear personnel responsibility, and maintain time-stamped hiring records protect themselves not only from regulatory enforcement but from the class action exposure that develops when urgency is used as a systematic reason to skip required steps.
At minimum, urgent healthcare hires require an OIG LEIE exclusion check before the worker provides any billable service, primary source license verification before clinical care begins, and a criminal background check ordered under a complete FCRA disclosure and authorization process. SAM.gov exclusion searches apply to facilities with federal contracting relationships. State law may impose additional requirements including abuse registry checks and sex offender registry searches. State criminal history reporting rules also vary by jurisdiction and should be confirmed with a PBSA-accredited background check provider.
Yes. FCRA applies to any consumer report procured for employment purposes, regardless of whether the position is temporary, per-diem, contract, or permanent. Urgency, short assignment duration, and agency placement do not create any FCRA exception. Disclosure, authorization, and adverse action procedures apply in full. Both the placing agency and the receiving facility may carry independent FCRA obligations depending on which entity orders the consumer report.
Generally, no. Civil Monetary Penalty liability arises at the point of employment or service provision, not at the point of audit or discovery. A limited emergency exemption exists under federal regulations for certain emergency items or services not provided in a hospital emergency room, but this exemption is narrow, does not apply to routine urgent staffing scenarios, and should not be relied on without legal counsel review. The LEIE search at exclusions.oig.hhs.gov takes under five minutes per individual.
The facility retains its own independent obligation to verify OIG exclusion status and primary source licensure regardless of what the agency has screened. The facility is the entity subject to CMS survey and Joint Commission accreditation, and its own verification documentation must exist in its credentialing files. Agency screening supplements but does not replace the facility's independent duty. SAM.gov and LEIE checks are non-delegable obligations for the facility.
With parallel sequencing, the mandatory elements of a healthcare background check can be initiated within minutes of a verbal offer. OIG LEIE results are immediate. Nursys license verification for RNs and LPNs returns results in real time. Criminal background check turnaround depends on the counties searched and court record availability, but digital authorization processes eliminate the authorization lag that accounts for much of the delay in traditional sequential workflows.
The facility is subject to Civil Monetary Penalties on a per-item or per-service basis, plus potential assessments of up to three times the amount claimed, under the applicable federal statute. Penalties can accumulate significantly when an excluded individual has provided multiple billable services before discovery. Voluntary self-disclosure to the OIG may reduce penalties but does not eliminate liability. Consult legal counsel promptly if an exclusion is discovered after placement.
State laws impose a range of restrictions on what criminal history information can be included in a background check report, including lookback period limits, restrictions on reporting non-conviction records, and requirements that vary based on where the applicant resides, where the employer operates, or where the underlying record originates. States including California, New York, Maryland, Massachusetts, Washington, and others have specific rules that can affect what a background check provider may lawfully report. Employers should work with a PBSA-accredited provider that applies current state-specific reporting rules.
Recruiter & Editor
Charm Paz is an HR professional at GCheck, specializing in background screening, fair hiring, and regulatory compliance. She holds from the Professional Background Screening Association (PBSA) and helps organizations navigate employment regulations with clarity and confidence.
With a background in Industrial and Organizational Psychology, she translates policy into practice to build ethical, compliant, human-centered hiring systems that strengthen decision-making over time.
Contact us today for efficient, FCRA-compliant screening solutions
designed to keep your hiring process moving safely and smoothly.


LEGAL DISCLAIMER: The information provided in this article is for general informational and educational purposes only and should not be construed as legal advice or a substitute for consultation with qualified legal counsel. While we strive to ensure accuracy, employment screening laws and regulations—including but not limited to the Fair Credit Reporting Act (FCRA), Equal Employment Opportunity Commission (EEOC) guidelines, state and local ban-the-box laws, industry-specific requirements, and other applicable federal, state, and local statutes—are subject to frequent changes, varying interpretations, and jurisdiction-specific applications that may affect their implementation in your organization. Employers and screening decision-makers are solely responsible for ensuring their background check policies, procedures, and practices comply with all applicable laws and regulations relevant to their specific industry, location, and circumstances. We strongly recommend consulting with qualified employment law attorneys and compliance professionals before making hiring, tenant screening, or other decisions based on background check information.