Hospital volunteer background check programs require layered screening protocols that distinguish between patient-facing and non-patient-facing roles, with intensity levels calibrated to access privileges and vulnerability of populations served. Healthcare administrators must balance Joint Commission accreditation standards, state-specific regulations, and institutional liability protection while implementing screening timelines that maintain volunteer pipeline efficiency without compromising patient safety integrity.
Key Takeaways Outline
- Hospital volunteer background checks must differentiate screening intensity based on direct patient contact, access to controlled substances, and interaction with vulnerable populations including pediatric and geriatric patients.
- Joint Commission standards require healthcare organizations to conduct background checks on all volunteers with patient contact or access to sensitive areas, though specific screening components remain at institutional discretion.
- Criminal history screening for healthcare volunteers should include county-level searches covering seven-year periods minimum, with federal database checks for roles involving Medicare/Medicaid patients or controlled substance proximity.
- Healthcare volunteer screening requirements extend beyond criminal records to include abuse registry checks, sex offender registry verification, and tuberculosis testing for patient-facing positions.
- Processing timelines for hospital volunteer background checks typically range from 5-14 business days depending on jurisdiction and screening depth, requiring volunteer coordinators to build buffer periods into orientation schedules.
- Patient-facing volunteer roles in pediatric units, oncology departments, and geriatric care facilities warrant enhanced screening protocols including child abuse registries and elder abuse databases at state levels.
- Healthcare institutions face direct liability exposure when inadequate volunteer screening results in patient harm, making comprehensive background check policies essential risk management tools beyond mere accreditation compliance.
- Volunteer background check policies must include clear disqualification criteria, individualized assessment frameworks compliant with Fair Credit Reporting Act requirements, and documentation retention schedules aligned with healthcare regulatory standards.
Understanding Hospital Volunteer Background Check Requirements
Healthcare facilities operate under heightened scrutiny regarding personnel screening due to the vulnerable populations they serve. The potential for significant harm from inadequate vetting has transformed volunteer screening from basic criminal checks to comprehensive systems. These systems now account for role-specific risks and regulatory expectations across multiple oversight bodies.
Regulatory Framework Governing Healthcare Volunteer Screening
The Joint Commission accredits approximately 88% of U.S. hospitals and establishes foundational standards requiring organizations to conduct background checks on potential staff members including volunteers. These standards appear in the Human Resources chapter, specifically addressing the need to verify credentials and conduct appropriate background investigations before individuals begin duties. Patient contact roles and positions with access to sensitive areas trigger mandatory screening requirements.
Federal regulations add layers of requirements particularly for facilities receiving Medicare and Medicaid reimbursements. The Centers for Medicare & Medicaid Services mandate checks against the Office of Inspector General List of Excluded Individuals and Entities for anyone with patient access or billing responsibilities. State-level requirements introduce additional complexity, with jurisdictions imposing varying mandates for abuse registry checks, fingerprint-based screening, and specific disqualification criteria.
“Trust is built long before the first interaction ever happens.” From what has been observed in practice, volunteer roles that are regarded as lower risk may still carry high responsibility, especially in regards to matters of patient access and access to sensitive areas. This indicates that role-specific recruitment methods are not only beneficial in protecting the organization, but also in protecting the dignity of the individuals we are serving. The best-run volunteer programs are the ones that are respectful enough to set standards.
Patient-Facing Versus Non-Patient-Facing Volunteer Distinctions
The most critical variable in hospital volunteer background check design involves the nature and extent of patient interaction. Patient-facing volunteers require substantially more intensive screening than individuals performing exclusively administrative or facilities support functions.
Patient-facing roles include volunteers who provide direct services in clinical environments:
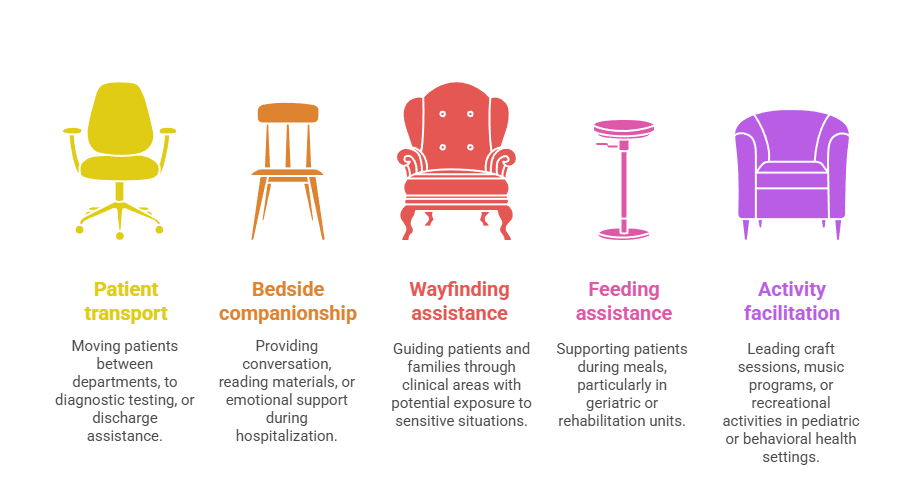
- Patient transport services: Moving patients between departments, to diagnostic testing, or discharge assistance
- Bedside companionship: Providing conversation, reading materials, or emotional support during hospitalization
- Wayfinding assistance: Guiding patients and families through clinical areas with potential exposure to sensitive situations
- Feeding assistance: Supporting patients during meals, particularly in geriatric or rehabilitation units
- Activity facilitation: Leading craft sessions, music programs, or recreational activities in pediatric or behavioral health settings
Non-patient-facing volunteers performing functions like gift shop operations, administrative filing in non-clinical areas, or fundraising event support present lower risk profiles. However, healthcare facilities must assess whether these roles provide incidental access to patient care areas, medical records systems, or pharmaceutical storage that would elevate screening requirements.
Essential Components of Healthcare Volunteer Screening Programs
Comprehensive hospital volunteer background check programs incorporate multiple verification layers, each addressing specific risk categories relevant to healthcare environments. Coordinators must understand which components apply universally versus those triggered by specific role characteristics.
Criminal History Searches for Hospital Volunteers
Criminal background screening forms the foundation of healthcare volunteer vetting, but the scope and depth require calibration based on role responsibilities. Most healthcare organizations implement county-level criminal searches covering jurisdictions where applicants have resided during the previous seven years. This timeframe aligns with Fair Credit Reporting Act guidelines for employment screening.
County criminal searches access courthouse records directly, capturing felony and misdemeanor convictions, pending charges, and disposition information. Healthcare facilities should prioritize these jurisdiction-specific searches over national database products that compile records from secondary sources.
| Search Type | Coverage Scope | Best Use Cases |
| County Criminal | Specific courthouse jurisdiction | All volunteers; primary screening foundation |
| Statewide Repository | State-compiled records | Supplements county searches in comprehensive programs |
| Federal Criminal | Federal court system | Roles with controlled substance access or Medicare/Medicaid patients |
| National Database | Secondary-source compilation | Initial broad screening only; requires primary verification |
Certain volunteer roles warrant federal criminal database searches, particularly positions involving Medicare or Medicaid patient populations or proximity to controlled substances. Federal searches capture offenses prosecuted in federal court systems including healthcare fraud, drug trafficking across state lines, and crimes on federal property.
Specialized Registry Checks for Healthcare Environments
Healthcare-specific databases add critical screening dimensions beyond general criminal history. The Office of Inspector General List of Excluded Individuals and Entities identifies persons barred from participating in federal healthcare programs due to fraud, patient abuse, or licensing violations. Volunteers with patient contact or access to billing systems require verification against this database.
Sex offender registries warrant checking for all patient-facing volunteer roles, with particular emphasis on positions involving pediatric populations or overnight shifts. The National Sex Offender Public Website aggregates registry data from participating jurisdictions, though state-level registry searches provide more current information.
Specialized abuse registries require verification based on vulnerable population exposure:
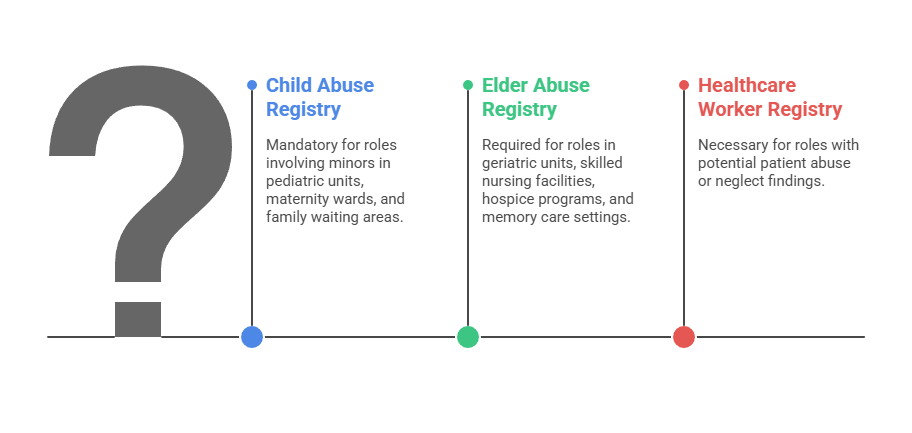
- Child abuse and neglect registries: Mandatory for pediatric units, maternity wards, family waiting areas, and any role involving minors
- Elder abuse registries: Required for geriatric units, skilled nursing facilities, hospice programs, and memory care settings
- Healthcare worker registries: State-maintained databases of individuals with substantiated patient abuse or neglect findings
These databases capture substantiated abuse reports that may not result in criminal convictions but indicate unsuitability for roles involving vulnerable populations.
Health Screening and Immunization Verification
Patient-facing hospital volunteers must complete health screenings equivalent to those required for clinical staff to prevent disease transmission. Tuberculosis testing through two-step purified protein derivative skin tests or interferon-gamma release assays provides baseline screening for infectious disease that could spread to immunocompromised patients.
Immunization verification ensures volunteers maintain current vaccinations for measles, mumps, rubella, varicella, tetanus, diphtheria, pertussis, and seasonal influenza. Healthcare facilities typically require documented proof of immunity through vaccination records or titer testing demonstrating adequate antibody levels. Additional health requirements may include hepatitis B vaccination series for volunteers with potential blood or body fluid exposure.
Implementing Risk-Based Screening Protocols
Healthcare institutions achieve operational efficiency and cost-effectiveness by calibrating hospital volunteer background check intensity to actual risk levels. A risk-based framework allows coordinators to allocate screening resources appropriately while maintaining patient safety standards.
Creating Volunteer Risk Classification Systems
Effective risk classification begins with systematic analysis of each volunteer position's characteristics. Patient contact type, vulnerable population exposure, access to medications or controlled substances, supervision levels, and duration of individual patient interactions all factor into risk assessment.
Healthcare organizations should establish three distinct risk tiers with corresponding screening protocols:
| Risk Level | Position Characteristics | Required Screening Components |
| High-Risk | One-on-one patient contact; unsupervised vulnerable population access; pediatric/geriatric care; medication proximity | Multi-jurisdiction criminal (7-10 years), federal database, all abuse registries, sex offender verification, detailed reference checks, health screening |
| Medium-Risk | Supervised group patient contact; wayfinding in clinical areas; administrative support with incidental patient information access | Statewide criminal search, sex offender registry, OIG exclusion check, basic reference verification, limited health screening |
| Low-Risk | No patient contact; no protected health information access; public areas only | Basic criminal search (county-level), sex offender registry, OIG exclusion verification |
High-risk volunteer positions typically include those providing one-on-one patient companionship, assisting with feeding or mobility, transporting patients between departments, or working in pediatric or neonatal units. Medium-risk positions involve supervised patient contact in group settings, wayfinding assistance in clinical areas, or administrative support in departments with incidental patient information access.
Screening Intensity for Pediatric Hospital Volunteers
Pediatric volunteer positions demand enhanced scrutiny due to the extreme vulnerability of child patients. Hospitals should implement automatic elevation to high-risk classification for any volunteer role involving children regardless of supervision levels.
Pediatric hospital volunteer screening protocols should extend beyond standard high-risk requirements. Criminal searches should cover all jurisdictions of residence for the previous ten years rather than standard seven-year periods. Child abuse and neglect registry checks must include verification in all states of prior residence, not just current location. Healthcare facilities serving pediatric populations should establish zero-tolerance disqualification criteria for any substantiated child abuse reports, any sexual offense regardless of conviction date, and any crime involving violence against minors.
Enhanced Protocols for Nursing Home Volunteer Screening
Long-term care facilities and hospital-based skilled nursing units require specialized screening attention due to residents' extended stays and cognitive vulnerabilities. Nursing home volunteer background check policies should incorporate elder abuse registry checks in all available jurisdictions, criminal searches emphasizing financial crimes and theft offenses that target vulnerable adults, and verification of any prior employment terminations from healthcare or caregiving positions.
Volunteers in memory care units or dementia-specific programs warrant additional scrutiny given residents' impaired ability to report concerns or identify perpetrators of abuse. These positions should require enhanced reference checking with detailed questions about patience, frustration tolerance, and prior experience with cognitively impaired populations.
Legal Compliance Frameworks for Healthcare Volunteer Screening
Hospital volunteer background check programs must navigate complex legal requirements that balance patient safety imperatives with applicant rights. Compliance failures expose healthcare institutions to regulatory penalties, accreditation challenges, and civil liability.
Fair Credit Reporting Act Requirements for Volunteer Screening
When healthcare facilities use third-party background screening companies to conduct volunteer background checks, the Fair Credit Reporting Act imposes specific procedural requirements. Institutions must provide clear disclosure that background checks will be conducted as a standalone document separate from the application. Written authorization from volunteer applicants must be obtained before initiating any screening activity.
Fair Credit Reporting Act compliance steps for healthcare volunteer screening:
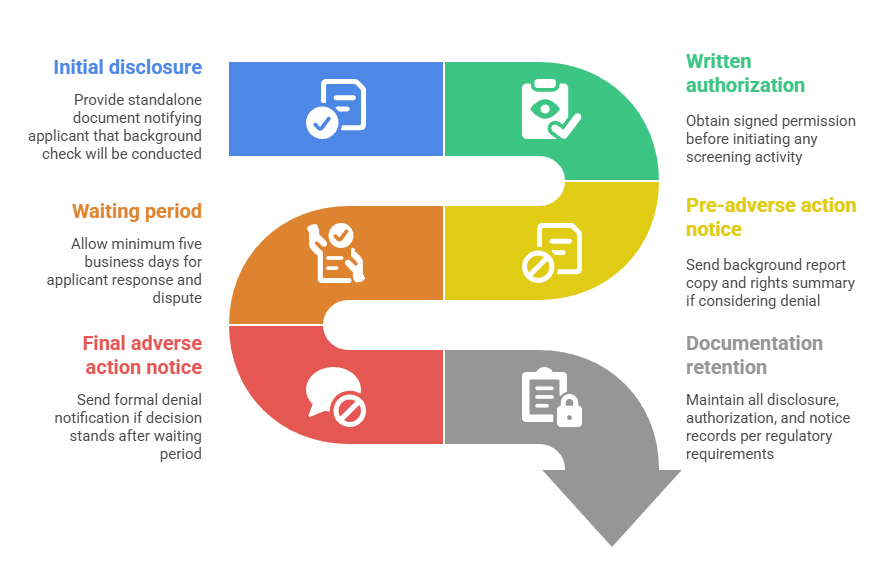
- Initial disclosure: Provide standalone document notifying applicant that background check will be conducted
- Written authorization: Obtain signed permission before initiating any screening activity
- Pre-adverse action notice: Send background report copy and rights summary if considering denial
- Waiting period: Allow minimum five business days for applicant response and dispute
- Final adverse action notice: Send formal denial notification if decision stands after waiting period
- Documentation retention: Maintain all disclosure, authorization, and notice records per regulatory requirements
Healthcare organizations conducting background checks using internal staff rather than third-party vendors may not trigger Fair Credit Reporting Act coverage. However, state-level consumer protection laws may impose similar requirements regardless of who performs the screening.
Individualized Assessment and Ban-The-Box Considerations
Healthcare facilities must implement individualized assessment processes when criminal history information emerges during volunteer screening. Blanket disqualification policies based solely on conviction existence without considering offense nature, time elapsed, or rehabilitation evidence may violate Equal Employment Opportunity Commission guidance.
Individualized assessment frameworks should evaluate the nature and gravity of the offense, the time elapsed since conviction or completion of sentence, and the nature of the volunteer position sought. Documentation of this analysis provides legal defensibility when screening decisions face challenge through administrative processes or litigation.
Documentation Retention and Privacy Protections
Healthcare institutions must establish retention schedules for volunteer background check records that balance regulatory requirements, accreditation standards, and privacy protections. Many facilities adopt seven-year post-separation retention aligning with general healthcare documentation standards.
Background check documentation containing sensitive information requires secure storage with access limited to personnel with legitimate need to know. Electronic systems should include audit trails tracking who accessed records and when, creating accountability and compliance evidence. Privacy protections extend beyond storage security to information sharing practices, with coordinators limiting disclosure of background check results to hiring decision-makers rather than broadly sharing findings.
Operational Implementation and Timeline Management
Successful hospital volunteer background check programs require strategic planning around processing timelines, applicant communication, and workflow integration. Volunteer coordinators must balance thoroughness with efficiency to maintain robust applicant pipelines.
Realistic Processing Timelines for Healthcare Volunteer Screening
Volunteer coordinators should build realistic timeline expectations based on screening scope and jurisdiction characteristics. Basic criminal background checks covering one or two counties typically return results within 3-5 business days when courts maintain electronic dockets. More comprehensive searches spanning multiple jurisdictions extend timelines to 7-10 business days for most applicants.
Average processing timelines by screening comprehensiveness:
- Basic screening (single county criminal, sex offender registry): 3-5 business days
- Standard comprehensive (multi-county criminal, federal check, abuse registries, OIG exclusion): 7-10 business days
- Enhanced screening (comprehensive criminal, all registries, detailed references): 10-14 business days
- Health clearance addition (TB testing, immunization verification, physical examination): Add 1-3 weeks to timeline
Healthcare facilities in jurisdictions with court backlogs or limited electronic access should anticipate longer timelines. Volunteer coordinators must communicate these timelines clearly during recruitment to set appropriate applicant expectations and reduce attrition during the screening phase.
Conditional Acceptance and Provisional Assignment Policies
Some healthcare institutions implement conditional acceptance frameworks allowing volunteers to begin limited duties in low-risk capacities while comprehensive background checks process. These policies require careful risk assessment, clear supervision protocols, and explicit documentation that assignments remain conditional.
Conditional assignments should restrict volunteers to non-patient-facing activities in non-clinical areas with direct supervision until full background clearance confirmation. Gift shop assistance under continuous staff oversight, administrative filing in public areas without protected health information access, and event setup tasks represent appropriate conditional assignment options.
Streamlining Processes for Seasonal and Event-Based Volunteers
Healthcare facilities hosting seasonal programs or special events requiring temporary volunteer surges face particular challenges balancing screening thoroughness with operational timelines. Event-based volunteer screening may justify abbreviated protocols when assignments involve no patient contact, occur in public spaces with continuous oversight, and last for single-day or weekend timeframes.
Abbreviated screening for short-term, low-risk volunteers might include sex offender registry checks, Office of Inspector General exclusion verification, and basic reference confirmation. Seasonal programs with recurring volunteers should implement annual rescreening protocols rather than full background checks for returning individuals whose previous screening occurred within the past year.
Building Defensible Disqualification Criteria
Healthcare organizations must establish clear disqualification standards that protect patients while providing legal defensibility and procedural consistency. Transparent criteria reduce coordinator discretion, support equitable treatment, and withstand scrutiny during accreditation reviews.
Absolute Disqualification Offenses for Patient-Facing Roles
Healthcare facilities should identify offense categories warranting automatic disqualification from patient-facing volunteer positions regardless of time elapsed or rehabilitation evidence. Clear communication of absolute disqualification criteria during recruitment prevents investment of time in screening applicants who cannot ultimately serve.
| Offense Category | Specific Examples | Disqualification Scope |
| Violent crimes against persons | Assault, battery, domestic violence, armed robbery | Permanent bar from all patient-facing roles |
| Sexual offenses | Any sex crime, possession of child sexual abuse material, registry presence | Permanent bar from all volunteer positions |
| Crimes against vulnerable adults | Elder abuse, financial exploitation, healthcare fraud | Permanent bar from geriatric care and positions with financial access |
| Patient abuse offenses | Healthcare worker abuse findings, OIG exclusions | Permanent bar from all healthcare volunteer roles |
| Homicide offenses | Murder, manslaughter, vehicular homicide | Permanent bar from all patient-facing roles |
Substantiated abuse reports in child or elder abuse registries should trigger automatic disqualification even absent criminal conviction. Presence on sex offender registries warrants permanent disqualification from any patient-facing volunteer role, with particular emphasis on positions involving children or overnight assignments.
Time-Limited Disqualifications and Rehabilitation Considerations
For offense categories not meeting absolute disqualification criteria, healthcare facilities should implement time-based exclusion periods allowing for rehabilitation demonstration. Property crimes without violence might warrant five-year disqualification periods from sentence completion. Drug possession offenses could justify three-year exclusions, while minor misdemeanors may require one-year waiting periods.
Rehabilitation evidence supporting individualized assessment decisions may include:

- Treatment program completion: Successfully finishing substance abuse treatment, anger management, or mental health programs
- Sustained employment: Maintaining consistent work history demonstrating responsibility and stability
- Educational achievement: Obtaining degrees, certifications, or professional training during the rehabilitation period
- Community service: Volunteering in non-healthcare settings showing commitment to positive community contribution
Healthcare facilities should document the specific rehabilitation evidence considered when accepting volunteers whose offenses fall within time-based exclusion windows.
Position-Specific Risk Tolerance Frameworks
Disqualification criteria should vary based on volunteer role risk levels identified through classification systems. Offenses resulting in automatic disqualification for high-risk patient-facing roles might permit consideration for low-risk positions without patient contact after appropriate exclusion periods.
Financial crimes including theft, fraud, and embezzlement warrant particular scrutiny for volunteers with access to patient valuables, payment processing, or donation handling. Drug-related convictions require careful analysis regarding volunteer assignment proximity to pharmaceutical storage, medication carts, or controlled substance documentation.
Continuous Monitoring and Rescreening Protocols
Initial hospital volunteer background checks provide point-in-time verification, but comprehensive programs include ongoing monitoring to identify issues emerging during service tenure. These protocols catch developments that occur after volunteers begin service and initial screening completion.
Annual Rescreening Requirements
Many healthcare accreditation standards and state regulations require periodic rescreening of volunteers at defined intervals. Annual rescreening represents best practice for patient-facing volunteers, balancing detection of new disqualifying information with administrative burden.
Annual rescreening typically includes criminal searches in the volunteer's current residence jurisdiction, reverification against Office of Inspector General exclusion lists and sex offender registries, and abuse registry checks where applicable. This focused approach captures new developments without duplicating comprehensive multi-jurisdiction searches conducted during initial screening.
Continuous Monitoring Technologies and Considerations
Some healthcare organizations implement continuous monitoring services that provide automated alerts when volunteers incur new criminal charges, convictions, or additions to exclusion databases. These systems offer real-time notification rather than waiting for annual rescreening cycles to detect disqualifying developments.
Continuous monitoring requires specific authorization from volunteers beyond standard background check consent, as it involves ongoing access to criminal justice databases. Healthcare facilities must ensure authorization documents clearly explain continuous monitoring scope and duration. While continuous monitoring provides enhanced protection, administrators should recognize that database coverage varies and alerts may not capture all relevant developments.
Self-Reporting Obligations and Disciplinary Integration
Volunteer policies should require immediate self-reporting of arrests, criminal charges, or convictions occurring during service tenure. Clear communication of this obligation during orientation and inclusion in volunteer agreements creates reporting expectations.
Healthcare facilities must integrate volunteer background check programs with incident reporting and disciplinary systems. Volunteer misconduct including policy violations, patient complaints, or concerning behaviors should trigger immediate review of continued service appropriateness. Coordination between volunteer services, risk management, and patient safety departments ensures comprehensive response to concerning incidents.
Conclusion
Hospital volunteer background check programs require sophisticated frameworks distinguishing screening intensity by risk level while incorporating healthcare-specific registry checks beyond general criminal searches. Healthcare administrators implementing these protocols must account for Joint Commission standards, federal exclusion requirements, and state-specific mandates while building operationally feasible timelines. Careful scrutiny and selection also further emphasize the point that the standards of care and accountability are applied to both volunteers and employees. This assists in providing a safer environment for healthcare stakeholders.
Frequently Asked Questions
What specific background checks are required for hospital volunteers under Joint Commission standards?
Joint Commission standards mandate background checks on volunteers with patient contact or access to sensitive areas, but specific screening components remain at institutional discretion based on role responsibilities. Most facilities interpret this as requiring minimum criminal history searches and healthcare exclusion database verification. Organizations should document their interpretation and ensure consistency between stated policies and actual screening practices.
How long does a typical hospital volunteer background check take to complete?
Hospital volunteer background check timelines typically range from 5-14 business days depending on screening scope and jurisdiction characteristics. Basic checks covering one or two counties with electronic court access usually complete within 5-7 business days, while comprehensive screening may require 10-14 business days. Health screening components including tuberculosis testing add 2-3 days for incubation and reading.
Do non-patient-facing hospital volunteers need the same background checks as patient-facing volunteers?
Non-patient-facing hospital volunteers typically require less intensive screening than those with direct patient contact, though specific distinctions depend on actual access to clinical areas and patient information. Volunteers working exclusively in gift shops or performing grounds maintenance may justify abbreviated screening focusing on basic criminal checks and registry verification.
What criminal convictions automatically disqualify someone from volunteering in a hospital?
Healthcare facilities typically establish automatic permanent disqualification for violent crimes against persons, any sexual offense, crimes against vulnerable populations including child or elder abuse, healthcare fraud or patient abuse, and homicide. Substantiated reports in abuse registries warrant disqualification even without criminal conviction. Other offense categories may justify time-limited exclusions ranging from one to five years from sentence completion.
Are pediatric hospital volunteers subject to different background check requirements?
Pediatric hospital volunteers warrant enhanced screening protocols due to child patient vulnerability, including extending criminal search timeframes from seven to ten years and conducting child abuse registry checks in all states of prior residence. Best practices include comprehensive sex offender registry verification and zero-tolerance disqualification policies for any offense involving children or any sexual crime.
Do healthcare facilities need to rescreen volunteers annually?
Many healthcare accreditation bodies and state regulations require periodic rescreening of volunteers at defined intervals, with annual rescreening representing best practice for patient-facing positions. Annual updates typically include criminal searches in current residence jurisdiction, reverification against healthcare exclusion lists and sex offender registries, and abuse registry checks where applicable.
Can hospitals allow volunteers to start while background checks are still processing?
Some healthcare institutions permit conditional volunteer assignments in limited low-risk capacities while a comprehensive background checks process, requiring careful risk management and clear procedural safeguards. Conditional assignments should restrict volunteers to non-patient-facing activities in non-clinical areas with direct continuous supervision such as gift shop assistance or administrative tasks.
What is the difference between county, state, and federal criminal background checks for hospital volunteers?
County criminal searches access courthouse records directly in specific jurisdictions providing the most accurate information for those geographic areas. Statewide searches query centralized state repositories that compile records from county courts, offering broader coverage but with varying completeness. Federal criminal searches access federal court system records, capturing offenses prosecuted federally including healthcare fraud and drug trafficking across state lines.
Do nursing home volunteers need to be screened differently than general hospital volunteers?
Nursing home volunteer screening should incorporate specialized components addressing unique vulnerabilities of long-term care residents including elder abuse registry checks in all available jurisdictions and criminal search emphasis on financial crimes targeting vulnerable adults. Enhanced protocols include detailed reference verification with specific questions about patience and experience with cognitively impaired populations.
What records must healthcare facilities maintain regarding volunteer background checks?
Healthcare organizations must retain documentation demonstrating completion of required background checks throughout volunteer service tenure plus periods specified in applicable laws and accreditation standards. Many facilities maintain volunteer screening records for seven years following service separation. Background check files require secure storage with access limited to personnel with legitimate need and audit trails in electronic systems tracking access.
Additional Resources
- The Joint Commission Human Resources Standards
https://www.jointcommission.org/ - Office of Inspector General List of Excluded Individuals and Entities
https://oig.hhs.gov/exclusions/ - Federal Trade Commission Fair Credit Reporting Act Guidance
https://www.ftc.gov/legal-library/browse/statutes/fair-credit-reporting-act - National Sex Offender Public Website
https://www.nsopw.gov/ - Centers for Medicare & Medicaid Services Regulations
https://www.cms.gov/

ABOUT THE CREATOR
GCheck Editorial Team
Meet the GCheck Editorial Team, your trusted source for insightful and up-to-date information in the world of employment background checks. Committed to delivering the latest trends, best practices, and industry insights, our team is dedicated to keeping you informed.
With a passion for ensuring accuracy, compliance, and efficiency in background screening, we are your go-to experts in the field. Stay tuned for our comprehensive articles, guides, and analysis, designed to empower businesses and individuals with the knowledge they need to make informed decisions.
At GCheck, we're here to guide you through the complexities of background checks, every step of the way.